






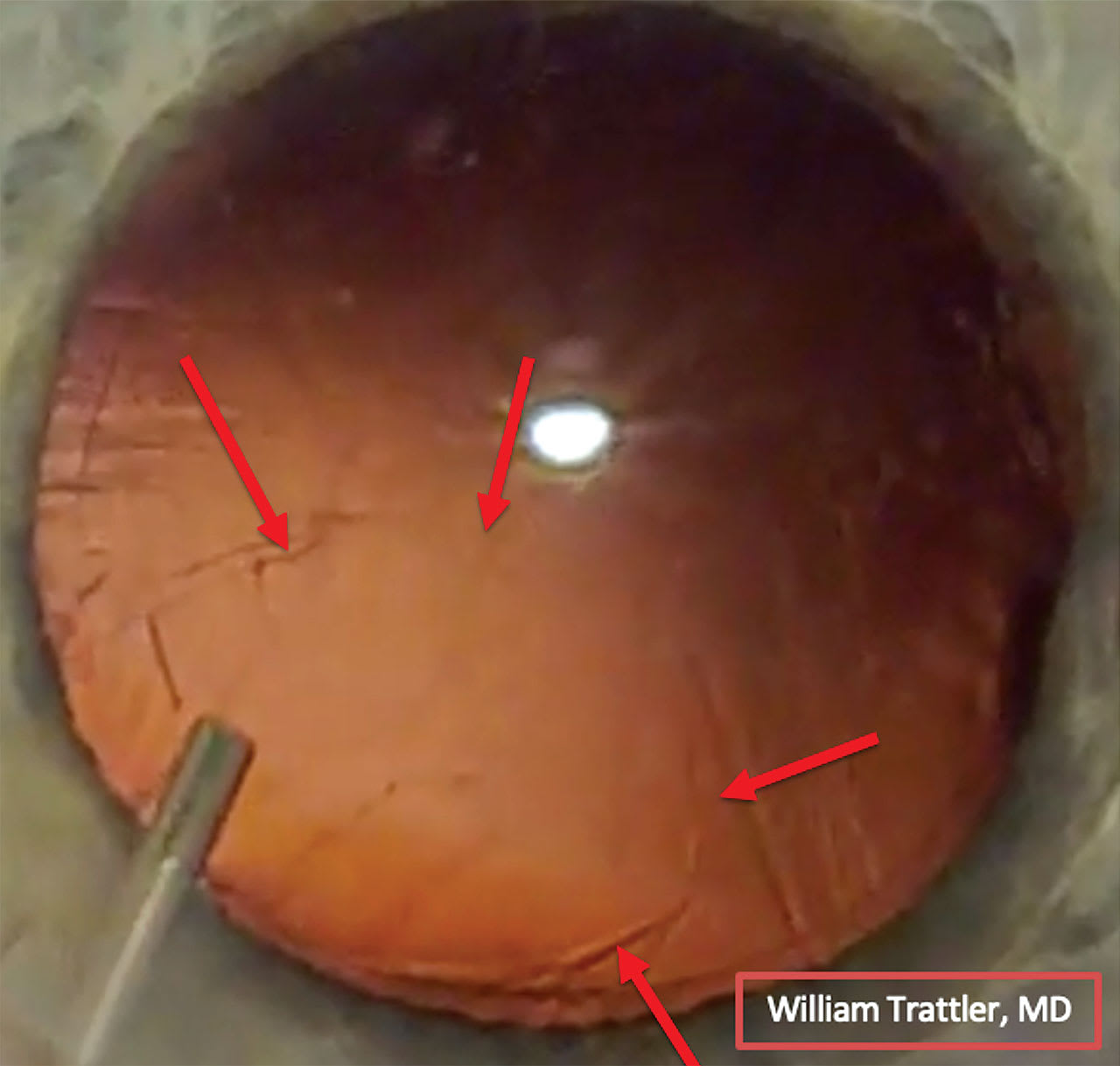
The patient is a 71-year-old man who is excited to receive a trifocal intraocular lens (IOL) (first eye). His wife previously had surgery with placement of trifocal IOLs, and she is very happy with her result. During cataract surgery, nuclear removal went smoothly. However, at the completion of cortex removal, a posterior capsular opening was identified (Figure 1). Viscoelastic was placed into the anterior chamber to prevent vitreous prolapse.
At this juncture, the surgeon must decide whether to proceed with placement of the trifocal IOL in the compromised capsule or to pivot to a different IOL technology.
QUESTION 1: Do you normally inform patients scheduled for a presbyopic IOL that there is a possibility that one cannot be placed?
QUESTION 2: In this particular case, how would you proceed? Please elaborate on your decision-making process.
MICHAEL VENINCASA, MD
Loh Ophthalmology Associates, Miami, FL
Indeed, I do routinely discuss with patients the potential need to place an alternate lens during cataract surgery. The lens discussion is an extremely important part of the preoperative consultation, because it allows the surgeon to understand the patient’s goals for postoperative vision and to set expectations regarding the various lens options. These discussions play a large role in postoperative success and patient happiness. The patient needs to be aware of operative risks and benefits as part of the informed consent process, and I see the lens discussion as a vital portion of this process. Although it is rare that we are unable to implant the planned IOL, this possibility is best introduced to the patient preoperatively in the clinic chair, rather than on the operating table or afterward.
In this case, the surgeon identified a posterior capsular opening during cortex removal and promptly injected viscoelastic to tamponade against vitreous prolapse. It appears that the cortex was successfully removed, and the posterior capsular opening is round, with an intact anterior capsule. If inspection reveals vitreous prolapse, I would proceed with a standard anterior vitrectomy.
However, because viscoelastic was promptly used here after identification of the posterior capsular opening, it is likely that there is an intact vitreous interface without prolapse. We can probably proceed to IOL implantation at this time. The posterior capsular opening is round, and the anterior capsule appears intact, so I would proceed with implantation of the planned 1-piece trifocal IOL. I would take care to avoid undue pressure during implantation to minimize viscoelastic loss, and I would orient the IOL haptics away from the capsular defect to allow for the most stable lens placement. Postoperatively, I would counsel the patient and closely monitor for intraocular inflammation and lens stability. Because the case was handled appropriately, the patient is likely to do very well, with a great postoperative result.
CRISTOS IFANTIDES, MD, MBA
Tyson Eye, Cape Coral, FL
This situation is tough because trifocal patients on average tend to have higher expectations from their cataract surgery. Even though we do normally inform patients who are scheduled for presbyopia-correcting IOLs that there is a small chance that this type of lens might not be able to be placed, it is still a difficult conversation to have if one cannot be placed.
In this particular case, I would consider initially doing a limited anterior vitrectomy through the paracenteses. If the vitreous remains posterior, I would possibly forgo this step. If the anterior capsule is small and intact, I would consider placing a trifocal lens using reverse optic capture with the haptics posterior and the optic anterior to the anterior capsule. We place the lens in this configuration as a secondary solution for patients bothered by dysphotopsia after cataract surgery, and so this approach is reasonable for primary placement of a trifocal in situations in which the posterior capsule is compromised. An important thing to note with this option is to ensure proper placement of the lens center within the visual axis. This placement is less of an issue if using a toric or standard IOL, with which placement on the center of the lens can be more forgiving as long as the astigmatic axis is aligned. This is especially true with aspheric lenses that have the same power from the center of the lens to the edge of the lens, as is the case with the Bausch + Lomb MX60 standard and toric lenses.
If the lens is poorly positioned using reverse optic capture, I would consider a 3-piece IOL (including the RxSight Light Adjustable Lens) with or without optic capture, with the haptics in the sulcus and the optic posterior to the anterior capsule. The conversation with the patient would then include a discussion about the inability to place the advanced-technology IOL, and a backup plan would need to be implemented.
DR. TRATTLER’S APPROACH
I am very happy with the thought processes and pearls provided by Drs. Venincasa and Ifantides. I agree with Dr. Venincasa that a single-piece multifocal IOL can be placed in the capsular bag in certain situations in which there is a limited opening in the posterior capsule. I also agree with Dr. Ifantides that a reasonable approach can be to place the trifocal IOL initially in the capsular bag and then elevate the optic out of the bag so that it is secured by the anterior capsule (reverse optic capture).
One of the first things to consider is the presurgical discussion with patients. In addition to discussing risks such as infection, glare, or halos, one can consider discussing with patients that there is a rare risk that the planned IOL cannot be placed. As both Drs. Venincasa and Ifantides discussed, the planned single-piece IOL can still be placed even when there is a posterior capsular opening. However, there are certainly situations in which there is compromised capsular support such that it is best not to place a single-piece trifocal IOL.
In this case, when the posterior capsular tear was identified, dispersive viscoelastic was placed before removal of the irrigation/aspiration handpiece. This step prevented vitreous prolapse through the capsular opening. At this point, with a stable anterior chamber, one can take a moment to inspect the capsule and decide whether to continue with the planned technology (single-piece trifocal IOL) or pivot to a 3-piece monofocal IOL.
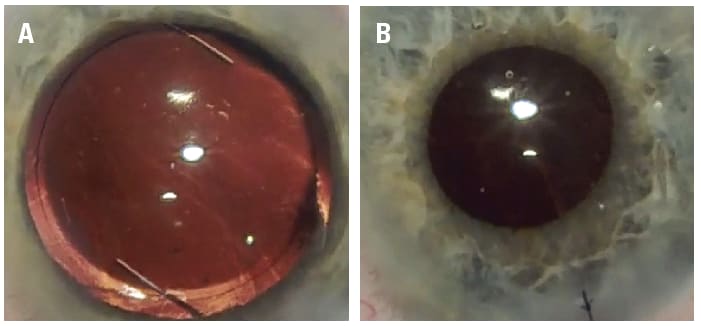
Further inspection revealed that the capsular tear also involved the anterior capsule. While careful placement of a single-piece IOL was still possible, I was concerned with centration. I decided to switch to a 3-piece silicone monofocal IOL (LI61AO by Bausch + Lomb) placed in the sulcus (Figure 2A). Following insertion, I was happy that I had a 3-piece IOL in the sulcus that appeared centered, and there was plenty of capsular support and no vitreous present. However, finishing these cases from this point can still be tricky.
I placed a 10-0 Nylon suture through the main incision (because I had enlarged it to 2.8 mm for insertion of the 3-piece IOL), and removed some of the viscoelastic with bimanual irrigation/aspiration. Removal of all of the viscoelastic can be a challenge because dispersive viscoelastic was used to protect the capsule before placement of the IOL. The anterior chamber was pressurized to a normal physiologic pressure, and then acetylcholine was used to constrict the pupil, followed by placement of 0.1% moxifloxacin in the anterior chamber. The pupil remained round, and there was no evidence of vitreous in the anterior chamber (Figure 2B).
The patient returned to our office for a same-day postoperative visit, our normal protocol for all cataract patients, and the IOP was found to be a little elevated. IOP-lowering drops were placed, and 45 minutes later, the IOP had returned to normal. The patient was instructed to continue their compounded triple-drop (prednisone-moxifloxacin-brimonidine), as well as use latanoprost at nighttime, since the IOP could still rise after the IOP-lowering drops placed in the office had worn off.
The most challenging part of the same-day postoperative visit was the discussion about why I did not feel comfortable proceeding with the planned trifocal IOL. The patient was disappointed, but was also understanding that the decision was appropriate based on the status of the capsule at the time of lens insertion. We also discussed that a trifocal IOL was still an appropriate option for the second eye and that most patients do very well even when only 1 eye has a trifocal IOL, and the other has a monofocal IOL.

Disclosures: Dr. Trattler is a consultant for Johnson and Johnson, Alcon, Bausch+Lomb, Zeiss, BVI, and Lensar. Dr. Ifantides is a consultant for Alcon, LENSAR, Zeiss, and Centricity Vision, and receives research support from Johnson and Johnson, and Bausch+Lomb. Dr. Venincasa has no relevant disclosures.